Definition: Any disturbance in rate, rhythm, or conduction of cardiac impulses deviating from normal sinus rhythm (60–100 bpm, regular, P before every QRS).
- AF affects ~46 million people worldwide
- Ventricular arrhythmias → ~300,000 SCDs/year (USA)
- Leading cardiac mortality cause in patients <40 years
- Prevalence rises sharply with age
- Sudden Cardiac Death – VF/VT most common cause
- Stroke risk – AF causes 20–30% of ischaemic strokes
- Heart failure – Tachycardia-induced cardiomyopathy
- Haemodynamic compromise – Syncope, shock
- Thromboembolism – AF mural thrombus
⚡ Davidson's Pearl: Haemodynamic stability is the primary determinant of urgency — always assess this before rhythm diagnosis.
- ARP: No stimulus excites (Phase 0–mid 3)
- RRP: Strong stimulus triggers AP (late Phase 3)
- R-on-T: Stimulus during RRP → VF risk ⚠️
SA Node: 60–100 bpm via If. AV Node: delays 120ms. Bundle of His → L/R bundles → Purkinje (20–40 bpm escape).
⚡ Golden Rule: Wide-complex tachycardia (QRS >120ms, rate >100) = VT until proven otherwise. Apply Brugada criteria.
- P wave – Atrial depolarisation. <120ms, <2.5mm
- QRS – Ventricular depolarisation. Pathological Q >1mm wide
- ST segment – Isoelectric. Elevation=STEMI, depression=ischaemia
- T wave – Ventricular repolarisation. Inversion=ischaemia/BBB
- Enhanced: Ischaemia, catecholamines, hypokalaemia → ectopic foci fire faster than SA node
- Suppressed: Vagal tone, drugs → sick sinus syndrome, bradycardia
- Abnormal Phase 4 slope in non-pacemaker cells
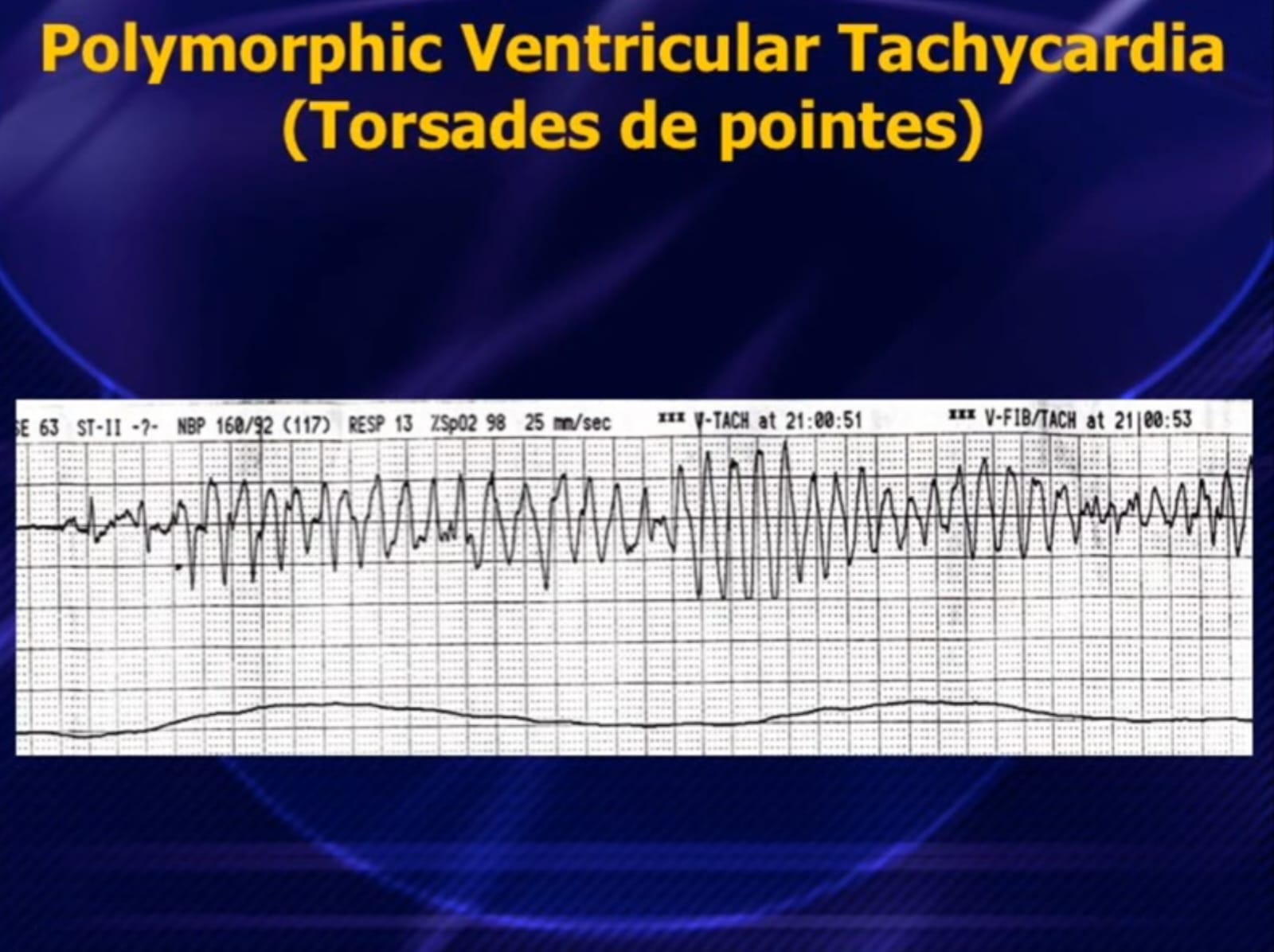
- EADs: Phase 2–3. Long QT, drugs, hypokalaemia → Torsades de Pointes
- DADs: Phase 4. Ca²⁺ overload → Digitalis toxicity, catecholamines
- Failure of impulse transmission: fibrosis, ischaemia, drugs, vagal tone
- Results: AV blocks (1°/2°/3°), BBB, SA exit block
Davidson's: Re-entry is the mechanism of most sustained arrhythmias. Catheter ablation targets and interrupts the circuit — basis of curative ablation.
- Sinus Tachycardia
- Atrial Fibrillation (AF)
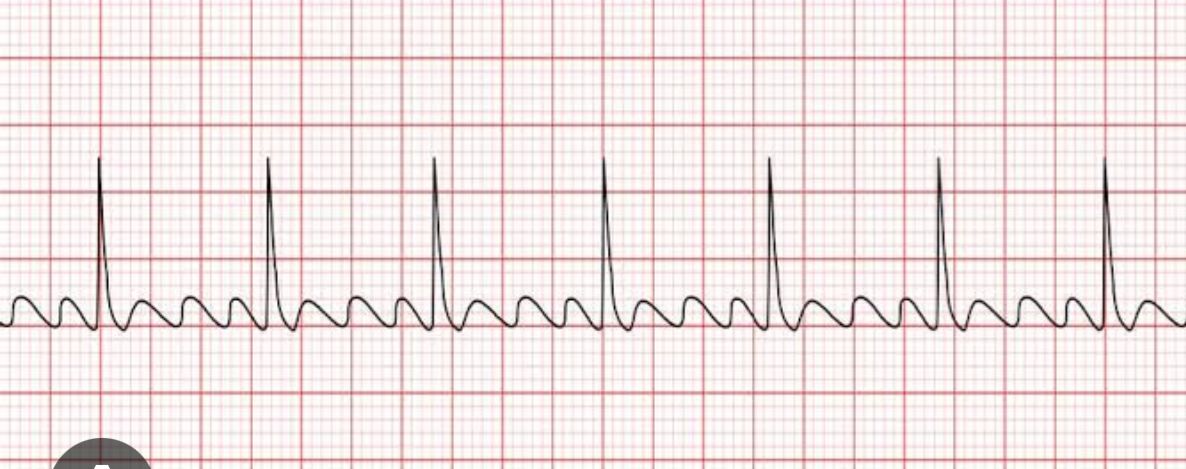
- Atrial Flutter
- Atrial Tachycardia
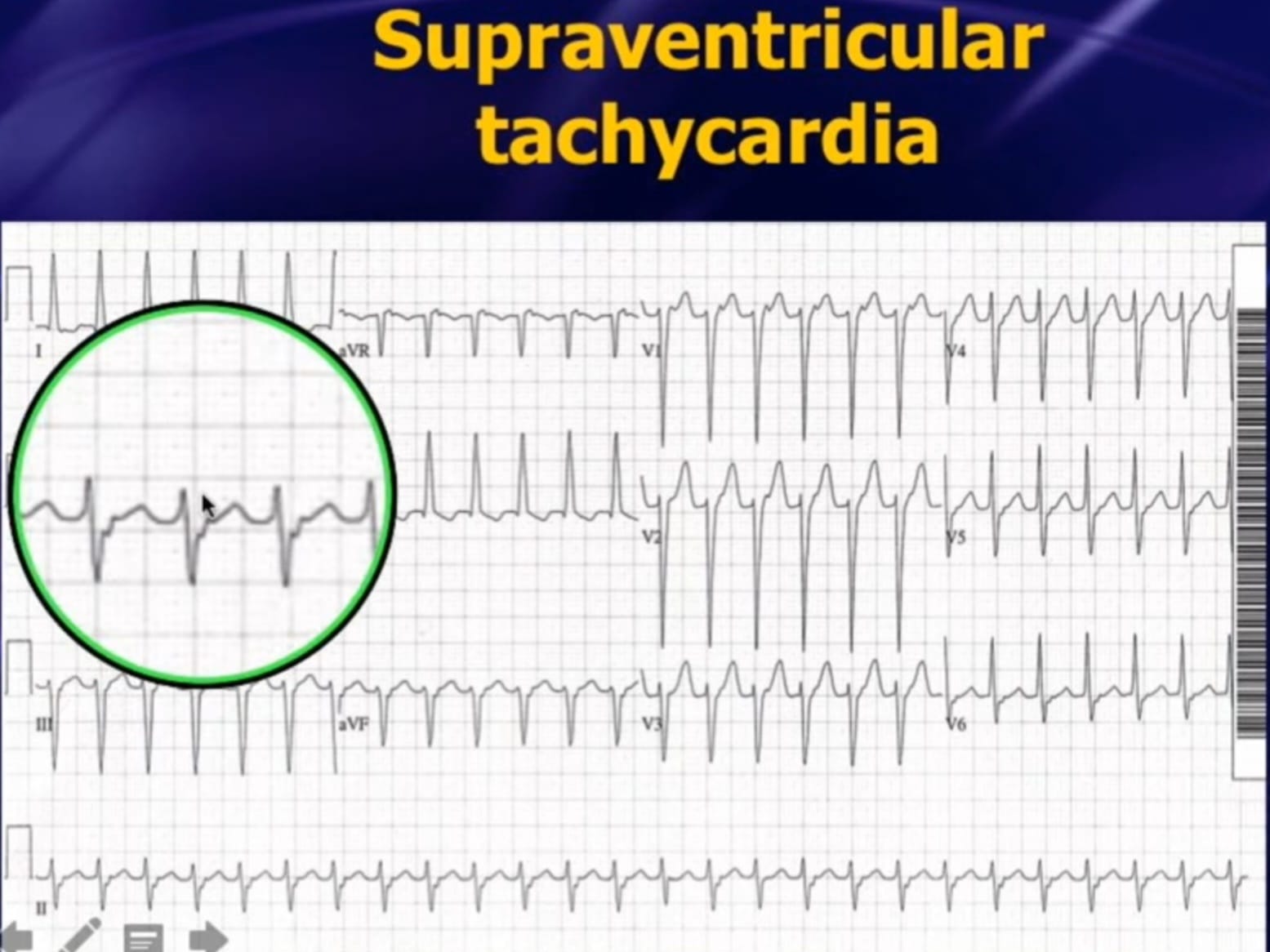
- AVNRT (most common SVT)
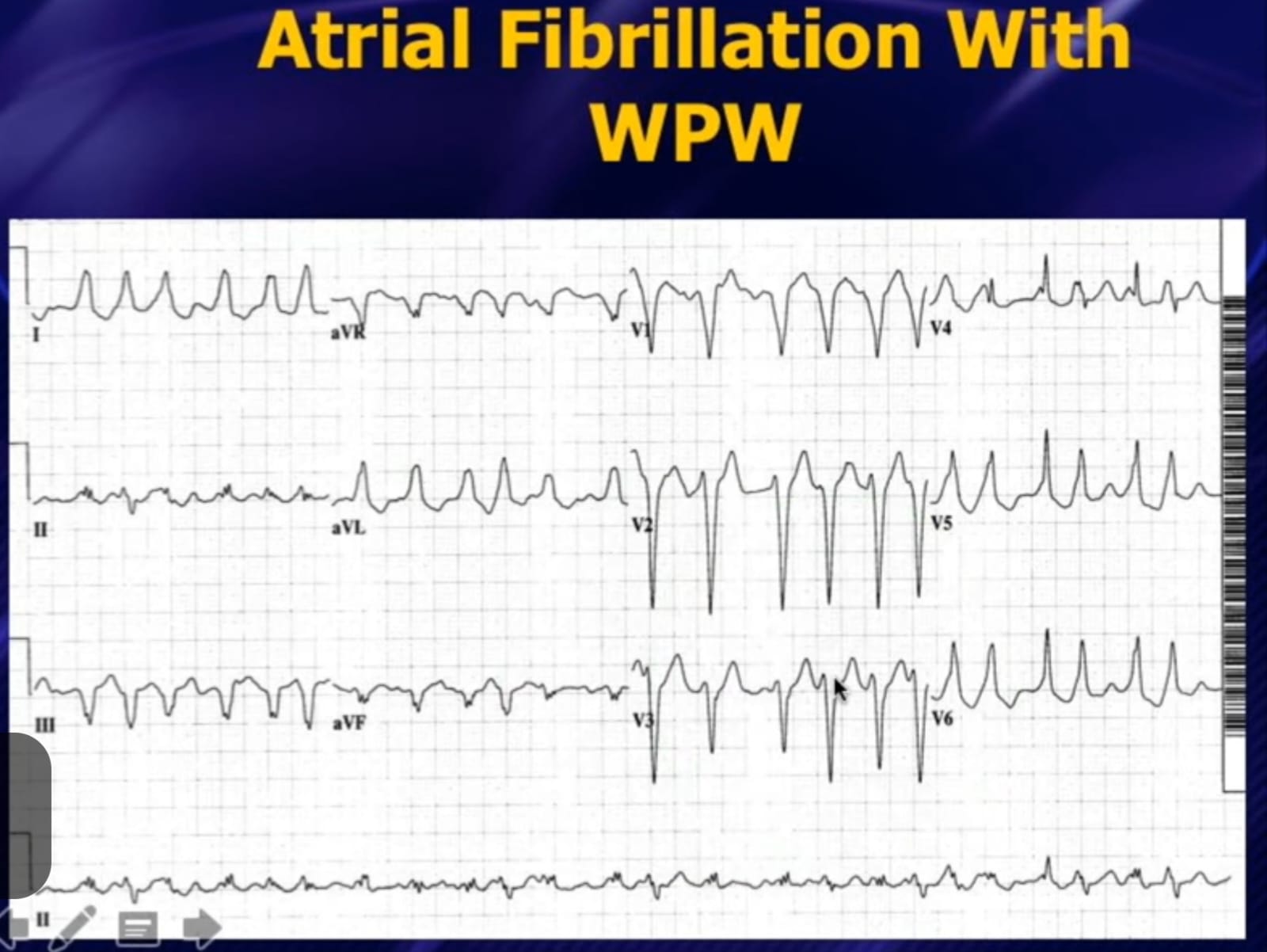
- AVRT (WPW syndrome)
- Junctional Tachycardia
- Sinus Bradycardia
- Sick Sinus Syndrome
- Premature Ventricular Complexes (PVCs)
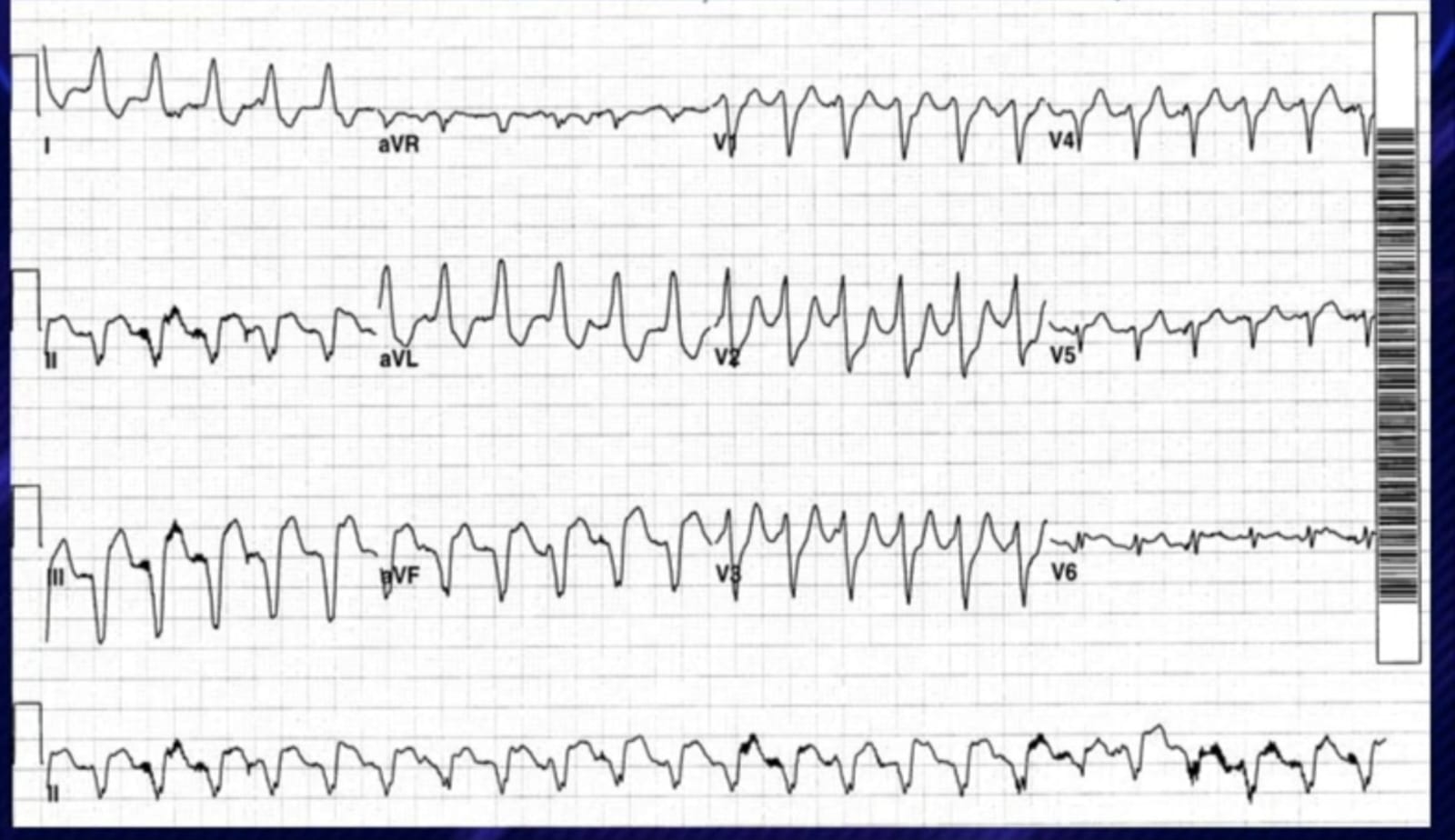
- Ventricular Tachycardia (VT)
- Sustained vs Non-sustained VT
- Monomorphic vs Polymorphic VT
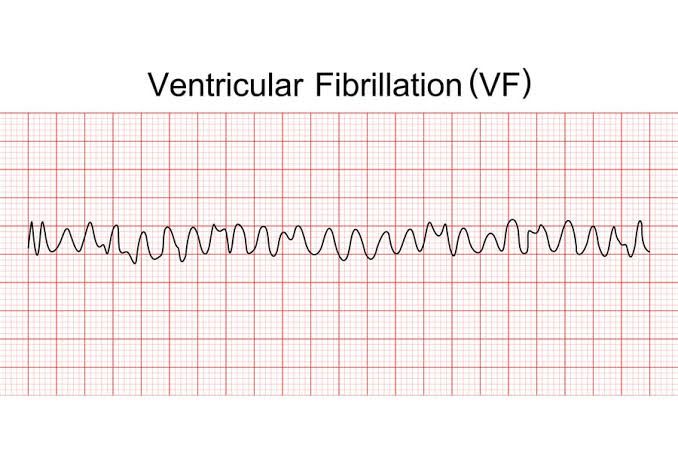
- Ventricular Fibrillation (VF)
- Torsades de Pointes
- Idioventricular Rhythm
- 1st Degree AV Block
PR >200ms, all conducted - 2nd Degree – Mobitz I
Wenckebach – progressive PR ↑ then dropped beat - 2nd Degree – Mobitz II
Sudden non-conducted P wave – dangerous! - 3rd Degree (Complete)
Complete dissociation – P & QRS independent
- RBBB / LBBB / Fascicular Blocks
- CHA₂DS₂-VASc ≥2(♂)/≥3(♀) → DOAC anticoagulation
- Rate control: β-blocker/diltiazem/digoxin <110 bpm
- Rhythm control: DCCV, flecainide (no structural disease), amiodarone
- Cavotricuspid isthmus ablation — >95% cure rate
- Rate/rhythm control as per AF guidelines
- Anticoagulate by CHA₂DS₂-VASc score
- Vagal manoeuvres → IV Adenosine 6mg bolus (terminates >90%)
- Alternative: IV Verapamil / β-blocker
- Unstable: Synchronised DCCV | Curative: RF ablation >98%
- AF+WPW: rapid accessory conduction → VF risk (200–300 bpm)
- Treat with IV Procainamide or DC cardioversion
- Definitive: Pathway ablation — curative
- Unstable: Synchronised DCCV 200J biphasic (sedate first)
- Pulseless VT: CPR + unsynchronised defibrillation
- Stable VT: IV Amiodarone 300mg over 20–60 min
- Correct K⁺ >4.5, Mg²⁺ >1.0 | Long-term: ICD if EF <35%
- CPR immediately (100–120/min, 5–6cm)
- Unsynchronised 360J mono / 200J biphasic
- Adrenaline 1mg IV every 3–5 min after shock 3
- Amiodarone 300mg IV after shock 3
- 4Hs & 4Ts reversible causes
- Congenital: LQT1 (KCNQ1), LQT2 (KCNH2), LQT3 (SCN5A)
- Drugs: Amiodarone, sotalol, quinidine, macrolides, antipsychotics
- Electrolytes: ↓K⁺, ↓Mg²⁺, ↓Ca²⁺
- Other: Bradycardia, hypothyroidism, intracranial events
- First-line: IV MgSO₄ 2g over 10 min (even if Mg²⁺ normal)
- Stop all QT-prolonging drugs immediately
- Correct K⁺ >4.5 mmol/L
- Overdrive pacing 100 bpm if recurrent
- Congenital LQTS: β-blockers (LQT1/2), ICD (high risk)
QTc >500ms = very high risk for TdP. Always check drug chart!
Management: 1° → observe | Mobitz I → monitor/treat cause | Mobitz II & 3° → IV Atropine bridge → Permanent Pacemaker (Class I indication)
- Palpitations – regular fast (SVT), irregular (AF), missed beats (ectopics)
- Syncope – Stokes-Adams (complete block), exertional (VT/HCM) = RED FLAG
- Pre-syncope/Dizziness – reduced cardiac output
- Chest pain – tachycardia-induced ischaemia
- Dyspnoea – haemodynamic compromise, decompensated HF
- Asymptomatic – incidental (PVCs, 1° AVB, paroxysmal AF)
⚡ Red Flags: Exertional syncope · Family history SCD · Structural heart disease · Syncope without prodrome · Wide complex tachycardia
Always correct: K⁺, Mg²⁺, thyroid, drugs, ischaemia before escalating treatment.
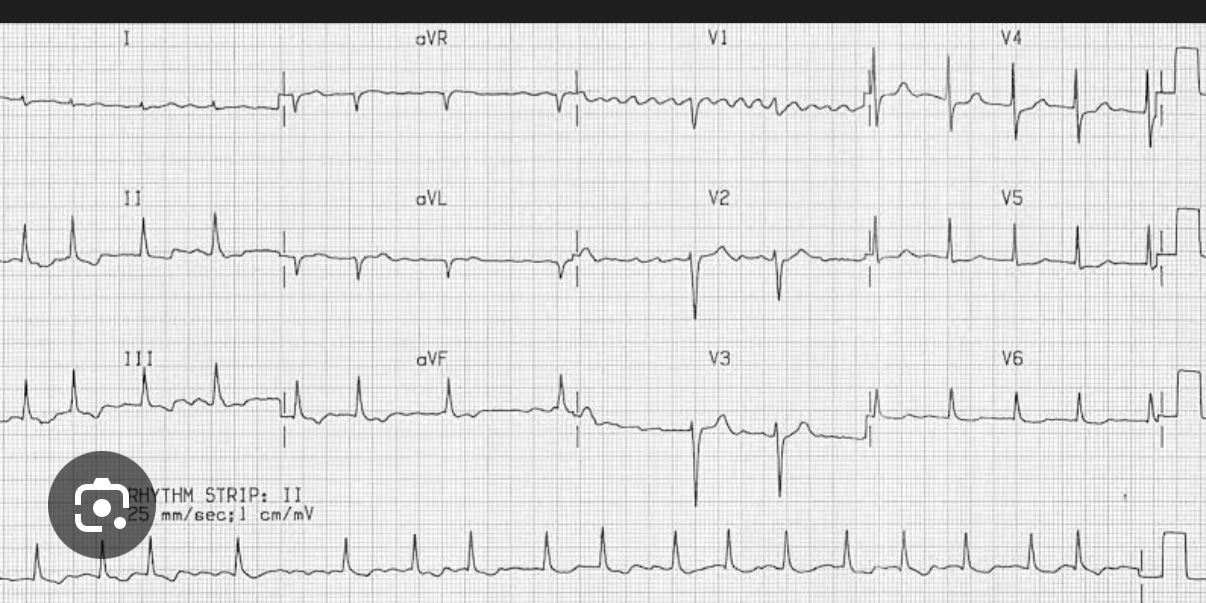
- Diagnosis: New-onset AF — absent P waves, irregular narrow QRS, f-wave baseline
- Precipitants: Hyperthyroidism (TSH low) + alcohol — both reversible
- CHA₂DS₂-VASc: Age(1)+HTN(1)+DM(1) = 3 → DOAC strongly indicated (apixaban)
- Mx: Rate control (bisoprolol 2.5mg), DOAC, treat hyperthyroidism, TTE, consider cardioversion after 3wk anticoagulation
- Davidson's Principles & Practice of Medicine, 23rd Ed. Elsevier 2022
- Braunwald's Heart Disease, 12th Ed. Elsevier 2022
- Kumar & Clark's Clinical Medicine, 10th Ed. 2022
- Hurst's The Heart, 14th Ed. McGraw-Hill 2022
- ESC AF Guidelines 2020 – Van Gelder et al. Eur Heart J 2020
- ESC Ventricular Arrhythmia & SCD 2022 – Zeppenfeld et al.
- ESC Cardiac Pacing 2021 – Glikson et al.
- AHA/ACC/HRS SVT Guidelines 2015 – Page et al.
- AHA ACLS 2020 | Resuscitation Council UK 2021